|
Min P. Kim, MD, FACS
Vice-Chair of Department of Surgery, David M. Underwood Distinguished Professor of Surgery, Head, Division of Thoracic Surgery, Professor of Surgery and Cardiothoracic Surgery at Weill Cornell Medicine, Professor of Surgery and Cardiothoracic Surgery at Institute
of Academic Medicine
|
One of the major factors contributing to the continued improvement in outcomes in thoracic surgery has been the thoughtful adoption of new technology. Advances in surgical innovation have allowed
us to provide safer, less invasive, and more effective care for our patients. Among these innovations, the robotic surgical platform has been one of the most exciting developments in our field. Robotic technology enables surgeons to perform increasingly complex
operations through smaller incisions, which often translates into less pain, shorter hospital stays, and faster recovery for patients.
At Houston Methodist, we are proud that our approach to adopting new technology is always centered on one principle: providing the best possible care for our patients while maintaining patient
safety as the foundation of everything we do. Innovation is only meaningful when it improves outcomes and is introduced with careful preparation, rigorous training, and a commitment to excellence.
|
We are especially excited to highlight the outstanding work of Dr. Chihara, who led our team in performing the first robotic lung transplant at Houston Methodist Hospital. This achievement was
the result of months of preparation and dedication. Dr. Chihara and the team spent extensive time studying operative videos and practicing robotic lung transplantation techniques in simulation models at the MITIE training facility. We were also fortunate to
have one of the surgeons involved in performing the world’s first robotic lung transplant visit as our Grand Rounds speaker, sharing invaluable insights and guidance with our team during training sessions at MITIE.
Introducing robotic technology into one of the most complex procedures in thoracic surgery required extraordinary planning, collaboration, and discipline. Because of the team’s commitment to
preparation and patient safety, the program successfully implemented this groundbreaking approach. I am incredibly proud of the entire team for accomplishing such a remarkable milestone.
Today, Houston Methodist has performed the most robotic lung transplants in Texas, reflecting both the dedication of our surgeons and the strength of our multidisciplinary transplant team. This
accomplishment represents not only innovation, but also our unwavering commitment to advancing patient care and improving outcomes for those we serve.
I am deeply proud of what our team has achieved and excited for what the future holds as we continue to push the boundaries of thoracic surgery in a safe, thoughtful, and patient-centered manner.
Min P. Kim, MD, FACS
|
|
|
The Society of Thoracic Surgeons Recognizes Houston Methodist Hospital Esophagectomy Program with "Better than Expected" Rating
|
|
The esophagectomy program at Houston Methodist Hospital has been recognized by The Society of Thoracic Surgeons (STS) with a prestigious “Better than Expected” rating, a distinction achieved
by only a small minority of programs nationwide.
In most STS reporting cycles, the majority of centers receive an “As Expected” designation, reflecting outcomes consistent with national benchmarks. Only select programs demonstrate statistically
superior outcomes after rigorous risk adjustment and are awarded the “Better than Expected” rating. This designation reflects a high level of confidence that patient outcomes exceed expected national results.
This achievement represents years of multidisciplinary collaboration focused on continuous improvement in esophageal cancer care. Several major initiatives have contributed to these outstanding
outcomes, including refinement of surgical technique through adoption of a completely robotic esophagectomy program and expansion of perioperative optimization strategies.
A key component of this effort has been enrollment of patients into the Surgical Optimization Program (formerly prehabilitation) led by Dr. Dhala. The program emphasizes nutritional support,
physical conditioning, pulmonary optimization, and overall patient preparedness before surgery. Combined with minimally invasive robotic surgical approaches, these efforts have resulted in meaningful improvements in perioperative outcomes, patient recovery,
and overall quality of care.
The STS also recognized the lung cancer resection program with an “As Expected” rating, reflecting outcomes that continue to meet important national quality benchmarks. More broadly, the thoracic
surgery program has demonstrated sustained improvement over time through multiple quality and enhanced recovery initiatives.
One important contributor has been implementation of a digital chest tube drainage system throughout the thoracic surgery service. Adoption of this technology has reduced hospital length of
stay by approximately one day on average and increased the number of patients able to have chest tubes removed in the recovery room. These advances, together with continued refinement of robotic surgical techniques and expansion of Enhanced Recovery After
Surgery (ERAS) pathways, have further improved patient recovery and overall program performance.
These recognitions reflect the Division’s continued commitment to innovation, multidisciplinary collaboration, and delivering the highest quality thoracic surgical care to patients.
|
|
|
Advancing Esophageal Cancer Surgery Through Robotics
|
|
On March 18, 2026, Dr. Ray Chihara delivered a featured presentation on robotic esophagectomy at the Houston Methodist Minimally Invasive Surgery Symposium, highlighting the remarkable evolution
of this complex procedure and its transformative impact on patient care.
During his talk, Dr. Chihara reviewed the historical progression of esophagectomy from traditional open operations to today’s advanced robotic-assisted approaches. He discussed how innovations
in minimally invasive and robotic technology have fundamentally changed the surgical management of esophageal cancer by improving visualization, enhancing precision, and allowing surgeons to perform highly complex procedures through smaller incisions.
Dr. Chihara emphasized the significant benefits robotic esophagectomy has brought to patients, including reduced postoperative pain, shorter hospital stays, faster recovery, and lower complication
rates, while maintaining excellent oncologic outcomes. He also highlighted how enhanced dexterity and visualization provided by robotic platforms have expanded the ability to safely perform intricate dissections and reconstructions in the chest and abdomen.
The presentation reflected Houston Methodist’s longstanding commitment to innovation in thoracic surgery and its leadership in advancing robotic techniques for complex foregut and esophageal
procedures. Through years of experience and continuous refinement of surgical techniques, the program has helped drive improvements in patient outcomes and broaden access to minimally invasive approaches for esophageal cancer treatment.
Dr. Chihara’s presentation was well received by symposium attendees and underscored the important role of multidisciplinary collaboration, surgical innovation, and education in continuing to
advance the field of minimally invasive thoracic surgery.
|
|
|
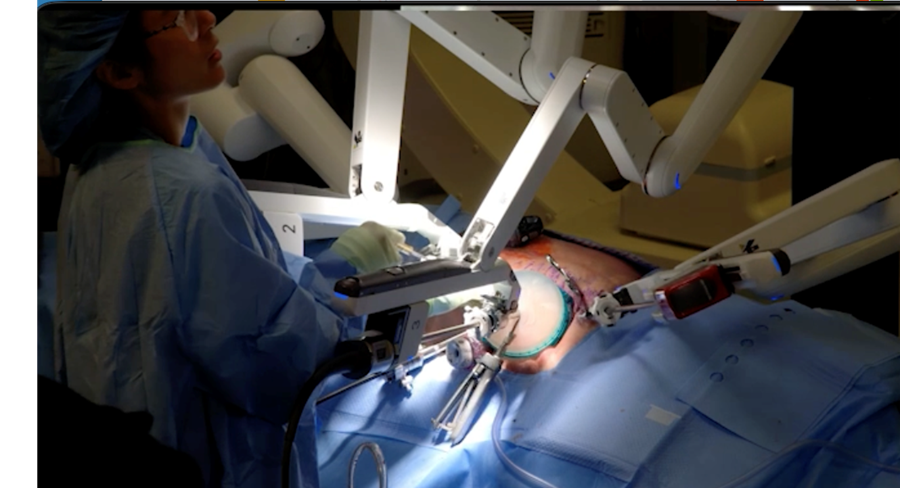
Robotic arms of the da Vinci Xi Surgical System, combining immersive 3D visualization with precise robotic instrumentation for advanced minimally invasive thoracic surgery
|
|
|
New Long-Term Data Suggest Durable Advantages of Heller Myotomy for Achalasia
|
|
Dr. Samar Semaan, research fellow in Division of Thoracic Surgery, presented important long-term outcomes research at the SAGES 2026 Annual Meeting in Tampa, with the study subsequently published
in Surgical Endoscopy. Guided by Dr. Min Kim, the presentation, titled “Comparative Long-Term Outcomes of Heller Myotomy and Peroral Endoscopic Myotomy,” evaluated the durability of two major interventions used to treat achalasia.
Achalasia is a rare esophageal motility disorder that can significantly impair swallowing and quality of life. Two commonly utilized interventions include Heller myotomy with fundoplication
and peroral endoscopic myotomy (POEM). While both procedures are effective in relieving dysphagia, limited data exist comparing their long-term outcomes.
|
Dr. Samar Semaan and
Dr. Min Kim
|
The study evaluated 172 patients who underwent intervention between 2013 and 2016, including 81 patients treated with Heller myotomy and 91 treated with POEM. Long-term patient-reported outcomes
were assessed using validated symptom questionnaires, including Eckardt, Dakkak Dysphagia, and GERD-HRQL scores, collected over multiple time periods between 2020 and 2025. One of the longest follow-up studies comparing these two interventions for achalasia.
Results demonstrated that both Heller myotomy and POEM provided durable long-term symptom control, with no significant differences in dysphagia or reflux-related quality-of-life scores between
the groups. However, important differences emerged in long-term management requirements. Patients undergoing POEM required significantly higher rates of proton pump inhibitor use and experienced a greater need for subsequent interventions, including dilation,
repeat myotomy, or esophagectomy. Intervention-free survival was significantly better in patients who underwent Heller myotomy with fundoplication.
These findings suggest that while both procedures achieve effective symptom relief, Heller myotomy with fundoplication may provide more durable long-term disease control with fewer additional
interventions and less dependence on reflux medication.
The presentation and publication reflect the Division’s continued commitment to advancing evidence-based esophageal surgery and contributing meaningful long-term outcomes data to the field of
foregut and minimally invasive surgery.
|
|
|
Pushing the Boundaries of Esophageal Reconstruction Through Multidisciplinary Collaboration
|
|
|
|
Dr. Chihara recently delivered an outstanding presentation at the annual Underwood Multidisciplinary GI/Surgery Grand Rounds, highlighting the complexity, innovation, and collaborative expertise
required to care for patients with advanced esophageal disease.
The presentation centered on a patient with a history of esophageal cancer who had previously undergone an esophagectomy and later developed a malignancy within the gastric conduit — a rare
and highly challenging clinical scenario. Dr. Chihara walked the audience through the patient’s complex treatment course, which required meticulous planning and coordination across multiple specialties.
|
The patient underwent an extensive operation to remove the cancer, followed by systemic chemotherapy and a delayed reconstruction utilizing a supercharged jejunal conduit. This highly specialized
reconstructive approach represents one of the most technically demanding procedures in foregut and thoracic surgery.
A major theme of the presentation was the importance of multidisciplinary collaboration in achieving successful outcomes for these extraordinarily complex patients. The operation required the
coordinated expertise of thoracic surgery, plastic surgery, surgical oncology, and ENT specialists, with each team contributing critical elements to the patient’s care and reconstruction.
Dr. Chihara emphasized that these procedures are not developed overnight, but rather through years of careful refinement, innovation, and institutional experience. The ability to offer advanced
reconstructive options such as supercharged jejunal reconstruction reflects the program’s long-standing commitment to pushing the boundaries of complex esophageal surgery while maintaining exceptional patient-centered care.
The case also showcased the strength of the multidisciplinary culture fostered through the Underwood Grand Rounds series, where collaboration across specialties continues to drive innovation
and improve outcomes for patients facing some of the most difficult surgical challenges.
Through presentations such as this, the Division of Thoracic Surgery continues to demonstrate its commitment to “Leading Medicine” by advancing complex surgical techniques and providing patients
access to highly specialized care that is available at only a select number of centers nationwide.
|
|
|
Advancing Lung Cancer Surveillance: Integrating ctDNA with Imaging
|
|
The Division of Thoracic Surgery continues to strengthen its commitment to innovation and excellence in cancer care through the expansion of its thoracic oncology surveillance program. For patients
with early-stage lung cancer who undergo curative surgical resection and do not require adjuvant systemic therapy, vigilant follow-up remains essential to ensure timely detection of recurrence.
Current surveillance guidelines from the National Comprehensive Cancer Network recommend routine imaging with CT scans—typically every six months for the first two years, followed by annual
scans thereafter. This approach has been effective in identifying recurrences at a stage when additional treatment can be offered.
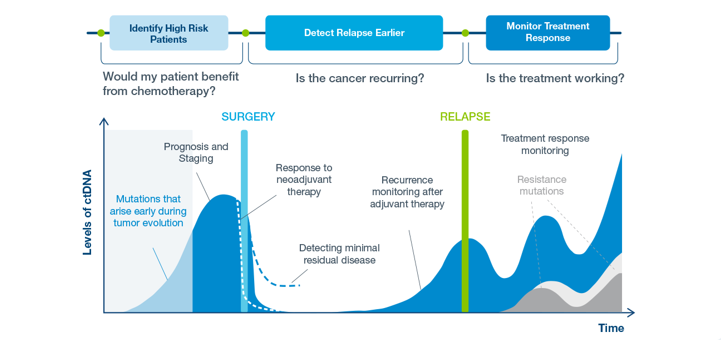
Building on this strong foundation, our division has incorporated a cutting-edge molecular tool into surveillance: circulating tumor DNA (ctDNA) testing. This technology analyzes tumor-specific
DNA fragments shed into the bloodstream, offering a highly sensitive and specific method to detect minimal residual disease and early recurrence.
Natera has developed a personalized, tumor-informed ctDNA assay known as Signatera. By sequencing a patient’s resected tumor, the test is customized to identify unique tumor mutations, allowing
for precise detection of recurrence through a simple blood draw. Unlike conventional imaging alone, ctDNA testing can be performed at shorter intervals, potentially identifying recurrence earlier and enabling more timely intervention.
Under the leadership of Dr. Min Kim, and with critical logistical coordination by Leo Meisenbach, our division has successfully implemented this program into clinical practice. The integration
of ctDNA surveillance alongside standard imaging represents a significant step forward in personalized cancer care.
This initiative exemplifies our mission to lead medicine—leveraging innovation, multidisciplinary collaboration, and precision technology to improve outcomes for our patients.
|
|
|
Texas Two Step: Improving Outcomes in Pulmonary Artery Sarcoma
|
|
|
|
Congratulations to
Dr. Warren Naselsky for his presentation at the AATS 2026 Annual Meeting, alongside
Dr. Marvin Atkins, titled “Texas Two Step for Pulmonary Artery Sarcoma-A Collaborative Approach.”
This work represents an important collaboration between cardiac and thoracic surgeons at Houston Methodist Hospital, focused on improving outcomes for patients with this rare and highly challenging
disease.
|
Traditionally, management of pulmonary artery sarcoma has required a combined procedure involving tumor resection from the heart via sternotomy along with pneumonectomy in a single operative
session. However, this approach has been associated with a significant risk of postoperative bleeding into the chest cavity.
The “Texas Two Step” approach introduces a staged strategy, separating the cardiac tumor resection from the pneumonectomy. This delay has led to a meaningful reduction in bleeding complications
and improved overall patient outcomes.
Importantly, leveraging our division’s expertise in advanced minimally invasive techniques, the pneumonectomy can now be performed using robotic technology. This innovation has further enhanced
the patient experience, contributing to faster recovery and improved perioperative outcomes.
This work highlights the strength of multidisciplinary collaboration and continued innovation in delivering cutting-edge care for complex thoracic diseases.
|
|
|
First Robotic Lung Transplant Performed at Houston Methodist Hospital
|
|
The Division of Thoracic Surgery at Houston Methodist Hospital successfully performed its first robotic lung transplantation, marking a major milestone in minimally invasive thoracic transplant
surgery. The program was led by Dr. Ray Chihara in collaboration with Warren Naselsky after months of structured preparation focused on patient safety and technical readiness.
Robotic lung transplantation is an emerging minimally invasive approach that may reduce postoperative pain, shorten recovery, and avoid large thoracotomy or sternotomy incisions. Given the complexity
and novelty of the procedure, the surgical team developed a comprehensive simulation-based training program before clinical implementation.
The multidisciplinary team — including thoracic surgeons, residents, and operating room staff — completed four cadaveric simulation sessions focused on robotic port placement, pneumonectomy,
and donor lung implantation. An experienced robotic lung transplant surgeon provided external technical guidance and institutional education through grand rounds and operative review.
The inaugural patient, who had end-stage emphysema and chronic respiratory failure, underwent bilateral lung transplantation using a carefully designed safety framework. The right lung was implanted
robotically through a 7 cm incision with additional port sites. As planned, the surgical team transitioned the second implantation to an open anterolateral thoracotomy approach to minimize graft ischemia time and prioritize patient safety. The patient tolerated
the operation without intraoperative complications and reported significantly less postoperative pain on the robotic side compared with the thoracotomy side.
This achievement reflects the Division’s commitment to innovation, multidisciplinary collaboration, and thoughtful implementation of advanced surgical techniques. The experience also highlights
the importance of simulation training, prospective safety planning, and disciplined intraoperative decision-making when introducing complex new procedures.
|
|
|
Grand Rounds Highlights Resident Perspective on Methodist's First Robotic Lung Transplant
|
|
On April 22, 2026, chief resident Therese Hoof delivered a Grand Rounds presentation titled
“From Simulation to Reality: Methodist’s First Robotic Lung Transplant,” offering a unique behind-the-scenes perspective on the development of Houston Methodist Hospital’s robotic lung transplant program.
The presentation highlighted the months of preparation, simulation training, and multidisciplinary collaboration that led to the institution’s first robotic lung transplantation performed by
Dr. Ray Chihara and the thoracic transplant team. Dr. Hoof shared her firsthand experience assisting in the creation and execution of the cadaveric simulation program that served as the foundation for the program’s safe clinical implementation.
Through her perspective as a resident, Dr. Hoof emphasized the critical role of education and structured training in advancing surgical innovation. She discussed how repeated simulation sessions
allowed the team to refine robotic docking, pneumonectomy techniques, donor implantation workflow, and intraoperative communication before performing the operation in a clinical setting.
The lecture also highlighted the importance of resident involvement in innovation and program development. By participating directly in simulation design, operative planning, and the inaugural
robotic transplant procedure, trainees gained valuable exposure to complex surgical problem-solving, multidisciplinary teamwork, and patient-centered decision-making.
Dr. Hoof’s presentation showcased how innovation in modern surgery extends beyond technology alone — requiring education, preparation, collaboration, and institutional commitment to patient
safety. Her reflections provided an important trainee perspective on one of the Division’s most significant recent surgical milestones.
Following completion of the general surgery residency program at Houston Methodist Hospital, Dr. Hoof will continue her training as a cardiothoracic surgery fellow at Vanderbilt University.
|
|
|
Welcome Emani Boyd, PA-C, to the Lung Transplant Team
|
|
The Division of Thoracic Surgery is pleased to welcome Emani Boyd, PA-C, to our lung transplant program, where she will work alongside Dr. Chihara and the multidisciplinary lung transplant team
to provide exceptional care for our patients.
Emani joins us with a strong background in cardiothoracic surgery and critical care medicine. Prior to joining Houston Methodist, she served as a Physician Assistant in Cardiothoracic Surgery
at ECU Health in North Carolina, where she cared for adult surgical patients in both inpatient and outpatient settings. Her experience includes perioperative management, advanced procedural skills, multidisciplinary care coordination, and participation in
complex thoracic surgical procedures including robotic and minimally invasive operations.
|
|
She also brings valuable critical care expertise from prior role in Pediatric Cardiac Critical Care at UT Health and Memorial Hermann, where she manages critically ill patients with congenital
and cardiovascular diseases requiring advanced hemodynamic monitoring, ventilator management, and ECMO support.
Emani earned her Master of Science in Physician Assistant Studies from South University and her Bachelor of Science in Biology with a Chemistry minor from the University of North Carolina at
Greensboro, graduating cum laude. She is board certified and maintains certifications in Advanced Cardiovascular Life Support (ACLS), Pediatric Advanced Life Support (PALS), and Basic Life Support (BLS).
Her dedication to patient-centered care, collaborative teamwork, and clinical excellence makes her an outstanding addition to our growing lung transplant program. We are excited to have Emani
join our team as we continue advancing innovative therapies and delivering world-class care to patients with advanced lung disease.
|
|
|
Meet our Thoracic Surgery Team
|
|
Min P. Kim, MD
mpkim@houstonmethodist.org
|
Ray K. Chihara, MD, PhD
rchihara@houstonmethodist.org
|
Warren C. Naselsky, MD, MS
wcnaselsky@houstonmethodist.org
|
Deven C. Patel, MD, MS
dcpatel@houstonmethodist.org
|
Left to Right: Dr. Ray K. Chihara, Dr. Deven C. Patel, Dr. Min P. Kim, Dr. Warren C. Naselsky
|
|